Is Sounding Safe? Sounding Safety Protocols & Risks
Is sounding safe? Yes, with sterile gear and slow technique. Learn the real risks (infection, tears, false passage) and the sounding safety protocols.
Yes — sounding is safe when you do it right: sterilize every sound, go slow, use plenty of sterile water-based lube, and pee afterward. The real risks — infection, a false passage or urethral tear from forcing, and object retention — are all preventable. Get the basics right and serious problems are genuinely rare.
Sounding is safe when you follow consistent protocols. The risks are real (infection, injury, and object retention all happen), but they're preventable. Every serious complication I've read about or heard of in the community traces back to skipping a basic safety step — or to believing one of the common myths about what's actually dangerous.
I've been sounding for about ten years. I've never had a UTI, never needed emergency care, and never damaged my urethra. That's not luck. It's protocol. This guide covers every safety layer I use before, during, and after every session, plus what to do if something goes wrong.
I'm not a doctor. This is harm-reduction education based on my personal experience and research. If something feels wrong, see a medical professional. No article replaces a doctor.
Equipment Safety
The safety of your session starts with what you put in your body. Not all sounds are created equal, and the wrong material can cause reactions, harbor bacteria, or physically injure the urethral lining.
Material Safety Profiles
Surgical-grade 316L stainless steel is the gold standard. It's what urologists use. It's non-porous, autoclavable, and chemically inert. If you're buying steel sounds, make sure the listing explicitly says 316L or surgical-grade. Just "stainless steel" could be anything.
Titanium is excellent: lightweight, hypoallergenic, and equally non-porous. It's more expensive and harder to find in sounding sizes. If you can get it, it's a great choice.
Medical-grade silicone is popular with beginners because it's flexible and less intimidating. It's body-safe, but it's porous at the microscopic level. That means it can't be fully sterilized the way steel or titanium can, and chemical sterilization degrades it over time. Replace silicone sounds regularly and never share them.
What to avoid: Anything with seams, rough spots, or visible imperfections. Chrome-plated mystery metals from unverified sellers. Glass (unless it's borosilicate from a reputable maker, and even then, inspect for cracks before every use). And absolutely nothing that wasn't designed for urethral insertion.
Here's an example of what should be tossed straight in the garbage. It'll scratch your urethra on each move.

Inspecting Your Sounds Before Every Session
Run your fingertip slowly along the entire surface of the sound before each use. Feel for nicks, pitting, rough patches, or any texture change. Check the tip especially. That's where defects cause the most damage.
Look at the surface under good lighting. Discoloration on steel can indicate corrosion. Cloudiness or tackiness on silicone means the material is breaking down. If anything feels off, retire the sound. A $30 replacement is always cheaper than a medical bill.
Sterilization Protocols
Sterilization isn't optional. It's not something you do "most of the time." Every single session, every single sound, every single time. The urethra has no protective barrier like skin does. Bacteria introduced directly into it have a near-straight path to the bladder. This is how UTIs happen. The CDC Guideline for Disinfection and Sterilization in Healthcare Facilities classifies instruments that enter sterile body spaces as "critical" items that require sterilization (not just disinfection), and moist heat under pressure is the most dependable method for heat-stable tools.
Boiling Method
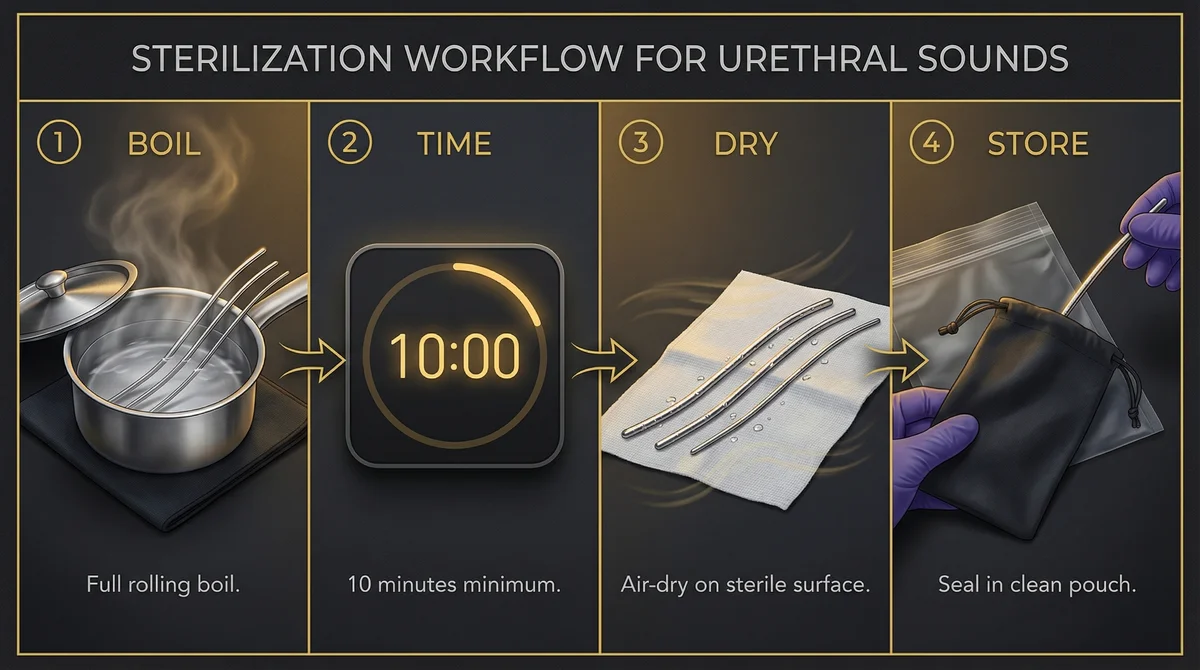
The simplest effective method. Submerge your steel or titanium sounds in a rolling boil for a full 10 minutes. Use a dedicated pot, not the one you cook pasta in. Let them air-dry on a sterile surface (a fresh paper towel or sterile gauze laid out on a clean plate). Don't towel them dry. Towels carry bacteria.
I keep a cheap stainless pot specifically for this purpose. It lives under the bathroom sink and has never touched food. Overkill? Maybe. But I've also never had a UTI from sounding.
Chemical Sterilization
For silicone sounds, travel situations, or when boiling isn't practical, a chemical soak works. Chlorhexidine solution or povidone-iodine (Betadine) are the go-to options. Submerge the sound for the time specified on the product: typically 10 to 15 minutes for chlorhexidine, or 2 minutes for a 10% povidone-iodine solution. Rinse with sterile saline or distilled water afterward.
Chemical sterilization is also your best option for silicone, since repeated boiling can degrade silicone over time.
What About Alcohol Wipes?
Isopropyl alcohol wipes are better than nothing, but they're not a sterilization method. Alcohol doesn't kill bacterial spores, and it evaporates before it can do a thorough job on a sound's entire surface. Use wipes for quick cleanup between insertions during a session, not as your primary sterilization step.
Storage After Sterilization
A sterilized sound re-contaminated by a dusty drawer is no longer sterile. Store sounds in a clean pouch, case, or zip-lock bag immediately after sterilization. Keep them in a dry place away from dust and moisture. Some practitioners use individual sterile barrier pouches, the same kind used in medical clinics.
Pre-Session Safety Checklist
Before the sound goes anywhere near your body, run through this checklist. It takes two minutes. I do it every time, even after ten years, because habits keep you safe when excitement makes you want to skip steps.
Personal Hygiene
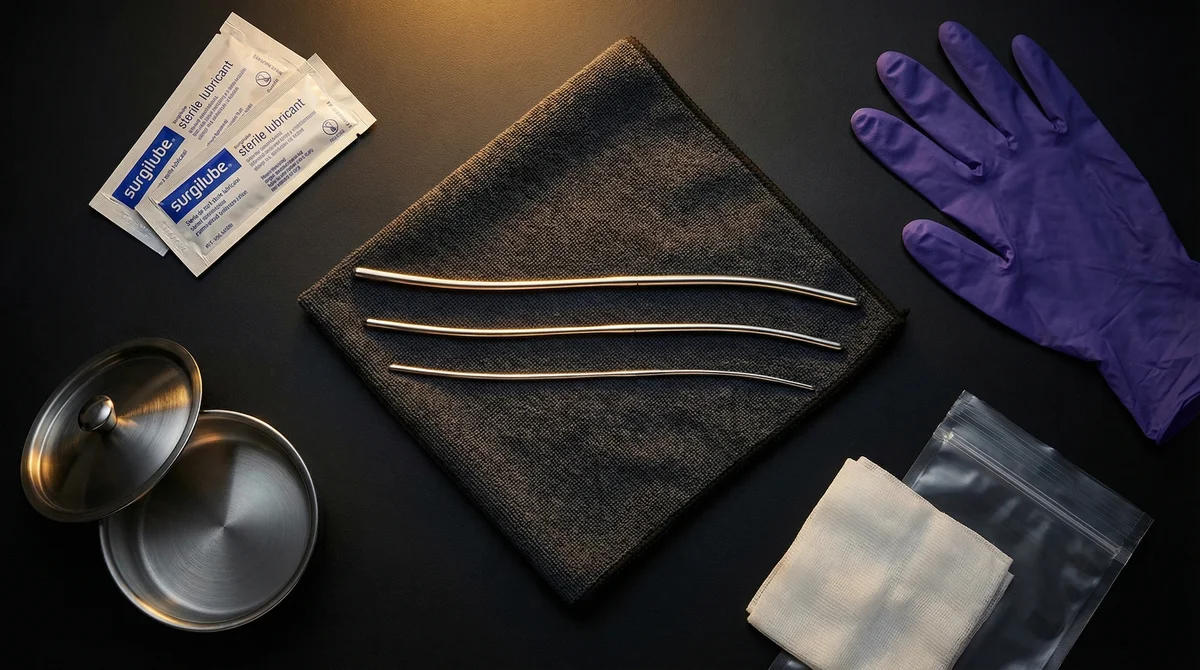
Wash your hands thoroughly with soap. Scrub for at least 20 seconds, the same way you would before handling a wound. Wash your genitals with warm water and gentle, unscented soap. Trim your nails short and smooth. Some practitioners wear nitrile gloves. I do when I'm sounding someone else, and it's a good habit for solo sessions too.
Lubrication: The Non-Negotiable
Use sterile, water-based lubricant. This is the one thing I'm going to be firm about. Not "water-based" from the bedroom drawer. Sterile lubricant that comes in sealed single-use packets, the kind you'd find in a medical supply store.
Why sterile? Regular lube can contain glycerin, parabens, or preservatives that irritate urethral tissue. It also isn't sterile, so bacteria from the tube opening get introduced directly into your urethra.
Why water-based? Silicone-based lubes can degrade silicone sounds. Oil-based lubes are difficult to flush out of the urethra and can trap bacteria. Water-based clears naturally when you urinate.
Never use numbing lube. You need to feel what's happening. Pain is your body's signal that something is wrong. Numbing that signal means you could push through tissue damage without realizing it.
The Clean-Hand Rule
One hand stays clean. The only thing it touches is the sound. Your other hand handles everything else: adjusting your body, spreading, repositioning, holding a mirror. Think of it like cooking: one hand touches raw chicken, the other handles everything else. Same logic, easy habit to build.
This applies whether you're solo or with a partner. If someone else is handling the sound, they follow the same rule: one dedicated clean hand on the instrument, nothing else. It's a small discipline that massively reduces contamination risk. For more on this in a female-specific context, see our female urethral sounding guide.
Environment and Mindset
Sound on a clean surface with good lighting. You need to see what you're doing. Bathroom or bedroom, doesn't matter, as long as the surface is clean and you're comfortable.
Don't sound when you're drunk, high, or exhausted. Impaired judgment leads to skipped steps, too much force, and delayed response to pain signals. Save it for when you're clear-headed and can pay attention to your body.
During-Session Safety
Insertion Technique Fundamentals
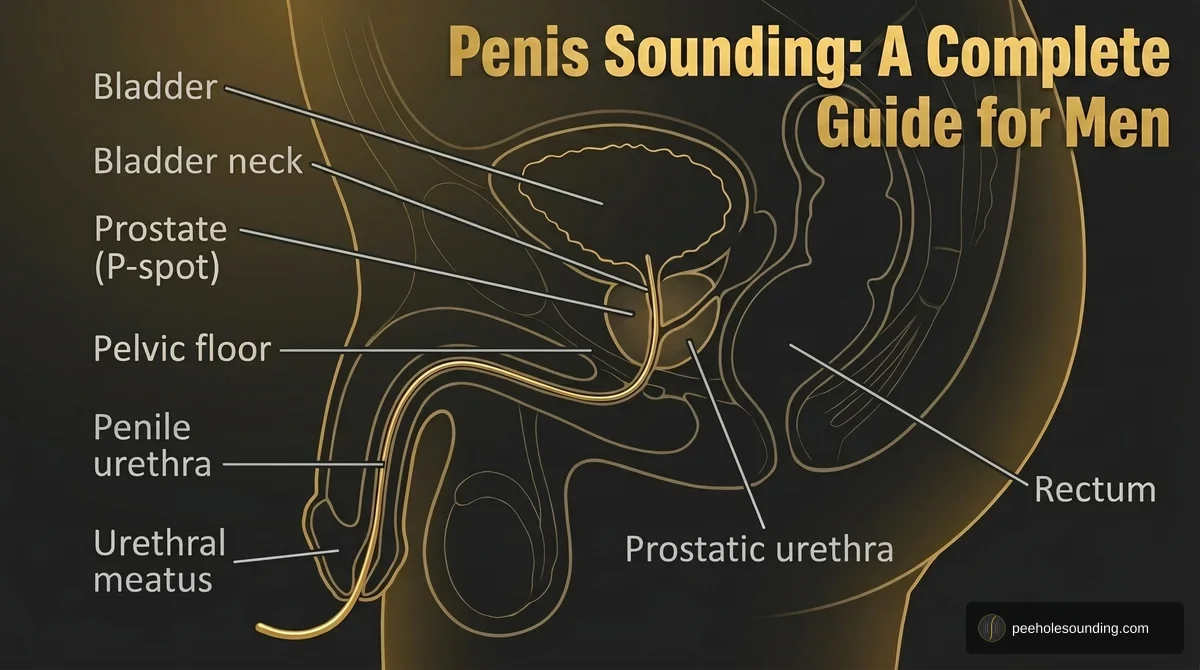
Hold the sound vertically and let gravity do the work. Never push a sound down with force. If it's meeting resistance, it's either the wrong angle, too dry, or too large. Add more lube, adjust the angle, or try a smaller size. (My step-by-step insertion guide covers angle and resistance points in detail.)
One thing that surprises beginners: don't start with the thinnest sound. Thinner sounds are actually more dangerous because they're more likely to puncture the urethral wall. Start with a sound that fits snugly but slides smoothly. For most people, that's somewhere around 1/8 to 3/16 inch. If you're not sure where to start, read the beginner's guide to urethral dilation for sizing guidance, or check out Hegar sounds — they're the standard graduated set most beginners reach for.
The Traffic Light System
This is the mental framework I use every session, and I recommend it to everyone:
Green: continue. The sound slides smoothly. You feel pressure, fullness, maybe a pleasant stretching sensation. Everything is gliding. This is where you want to be, and it's where most of the actual pleasure lives.
Yellow: pause and reassess. You hit unexpected resistance. You feel an unfamiliar sensation that isn't quite pain but isn't comfortable either. The sound stops moving. Stop. Don't push. Add more lube, adjust your angle, breathe and relax your pelvic floor. If yellow turns green, continue slowly. If it stays yellow, you're done for today.
Red: stop immediately. Sharp pain. Any amount of visible blood. Inability to pass urine. The sound won't move in either direction. Remove the sound gently (or leave it in place if it's truly stuck; see Emergency Protocols below), and do not continue the session. If symptoms persist, seek medical attention.
Partner Safety Considerations
If you're sounding with a partner, clear communication isn't optional. It's a safety requirement. Agree on a safeword before you start. The person being sounded should be the one calling the shots on depth, speed, and when to stop.
Never leave a sounded partner unattended. Don't combine sounding with restraint unless you're both experienced and the sounded person can always signal to stop. And the person doing the sounding should have clean, gloved hands and full control of the instrument at all times.
Aftercare Protocol
Immediate Steps
Urinate within 30 minutes of finishing your session. This is the single most effective way to prevent UTIs after sounding. Urine flushes bacteria out of the urethra before it can travel to the bladder. The NHS guidance on urinary tract infections emphasizes staying well hydrated and emptying the bladder promptly — especially after activity that can introduce bacteria to the urethra — as a core prevention step. Don't skip this. Even if you don't feel the urge, drink some water and wait.
Wash your genitals gently with warm water. Clean and sterilize your sounds before storing them. Don't leave them "for later."
24 to 72 Hour Monitoring
Some effects after sounding are normal. Mild stinging on the first urination? Totally expected, especially when you're starting out. A slight tingling sensation for a few hours? Also normal. These should fade within a day.
Watch for these warning signs:
- Burning that lasts more than 24 hours
- Cloudy or foul-smelling urine
- Blood in urine after the first post-session urination
- Fever or chills
- Difficulty urinating or a feeling of incomplete emptying
If any of these appear, see a doctor. Don't wait to see if it gets better. UTIs caught early are treated with a short course of antibiotics. UTIs that spread to the kidneys are a much bigger problem. Mayo Clinic's overview of hematuria also cautions that any visible blood in urine should be medically evaluated rather than self-monitored, even when it seems minor.
Is Sounding Safe? The Real Risks & How to Prevent Them
Infection and UTI Prevention
UTIs are the most common sounding complication, and they're almost entirely preventable. The recipe is simple: sterilize your sounds, use sterile lube, wash your hands, urinate after. If you do all four consistently, your UTI risk drops dramatically.
If you get recurring UTIs despite following protocols, talk to a doctor. Some people are more susceptible due to anatomy or underlying conditions. That's not a failure of technique; it's biology.
Physical Injury Prevention
The urethra is delicate tissue. Tears, abrasions, and in extreme cases perforation happen when people use too much force, use sounds with surface defects, or use objects that weren't designed for urethral insertion. The Urology Care Foundation's patient page on urethral trauma lists blood at the tip of the penis or in the urine, and inability to pass urine, as the signs of serious urethral injury that warrant immediate medical attention.
The prevention here is straightforward: never force a sound. If it doesn't slide smoothly with adequate lubrication, it's either the wrong size, the wrong angle, or your body is saying "not today." Listen.
Object Retention Prevention
Every ER case study I've read involving a lost object in the urethra has one thing in common: the person used something that wasn't designed for the purpose. Pens, wires, thermometers, magnets. A published review of urethral foreign body cases in PMC documents a wide range of self-inserted objects (pins, wires, ballpoint pens, screws) that required endoscopic or open surgical removal — reinforcing that improvised objects are the dominant risk factor for retention. Purpose-built sounds have flared ends, appropriate lengths, and smooth finishes specifically to prevent this.
Use only sounds designed for urethral insertion. Make sure the flared end or stop is secure and can't detach. Never use anything so small it could slip entirely inside. If you follow this, object retention is essentially a non-issue.
Emergency Protocols
When to Stop Immediately
Stop your session right away if you experience:
- Sharp, sudden pain (not mild pressure or fullness, but actual pain)
- Any visible blood on the sound or in urine during the session
- A sound that won't move in either direction
- A sudden burning sensation that wasn't there before
- Any loss of sensation or numbness
What to Do If a Sound Gets Stuck
Don't panic. A sound that won't move usually means your pelvic muscles have tightened around it. This is your body's reflex, and it's temporary.
First: Stop pulling. Take slow, deep breaths. Relax your pelvic floor, the same muscles you'd release to start urinating. Apply more sterile lube around the sound's entry point.
Second: Wait a few minutes. As your muscles relax, the sound should become mobile again. Try very gentle, slow rotation (not pulling) to break the seal.
Third: If it still won't move after 15 to 20 minutes of calm, patient attempts, go to the emergency room. Do not wait longer. Do not try to force it.
When to Go to the Emergency Room
Go to the ER if:
- A sound is stuck and won't move after gentle attempts
- You cannot urinate after removing a sound
- There is persistent or heavy bleeding
- You develop fever with urinary symptoms
- You have severe, worsening pain
How to Talk to Medical Professionals
Be honest. Say exactly what happened: "I was using a urethral sound and..." That's it. ER doctors and urologists have seen this before. You are not the first person to walk in with this, and you won't be the last.
The medical team needs accurate information to help you. Telling them what material the sound is made of, how long it's been stuck, and whether you've noticed blood or difficulty urinating gives them what they need for the best outcome. Embarrassment fades. Complications from delayed treatment don't.
Who Should Not Practice Sounding
Some conditions make sounding significantly riskier. If any of the following apply to you, talk to a doctor before sounding, or skip it entirely:
- Active UTI or urinary symptoms: you're adding instruments to an already-compromised system
- Immunocompromised: reduced ability to fight infections makes UTI risk much higher
- Pregnant: UTIs during pregnancy carry additional risks
- Known urethral stricture: structural narrowing requires medical management, not self-dilation. The Urology Care Foundation's overview of urethral stricture disease notes that prior urinary-tract instrumentation is itself a documented cause of strictures, so existing narrowing should be evaluated by a urologist before any further insertion
- On blood thinners: increased bleeding risk from even minor abrasions. Consult your prescribing doctor
- Under the influence: this isn't a medical condition, but impaired judgment makes every protocol harder to follow. Sound sober
If you're unsure whether a medical condition or medication interacts with sounding, ask your doctor. You don't have to explain why. "I'm considering urethral dilation and I take [medication]" is enough. If you want guidance on that conversation, check out our guide on what urethral sounding is for more context on the practice.
Frequently Asked Questions
Related Guides

What Is Urethral Sounding? A Complete Guide to Safety, Pleasure & Getting Started
Feb 15

Urethral Sounding for Beginners: Sizes & First Session
Apr 5

Sounding Pleasure: What It Feels Like & Why People Chase It
Feb 22

Female Urethral Sounding: Beginner Techniques & Safety
Mar 30

How to Insert a Urethral Sound (Step-by-Step)
Mar 25
How to Clean and Sterilize Urethral Sounds
Mar 20

Sounding Toy Guide: Types, Materials & How to Choose
Mar 10

Urethral Stretching Guide: Safe Progressive Dilation for Beginners
Apr 24
Penis Sounding for Men: Sizes, Safety & Prostate Technique
May 9

Sounding Myths Debunked: 10 Misconceptions That Keep People From Exploring Safely
Mar 1